Pudendal Neuralgia
Authors
INTRODUCTION
Pudendal neuralgia was first described in 1987 by Amarenco et al.1 It is a severely painful and disabling neuropathic condition, affecting both men and women, involving the dermatome of the pudendal nerve. This leads to pain in the clitoris/penis, vulva/scrotum, perineum, and rectum, especially when sitting. It has also been described as Alcock’s canal syndrome,2 cyclist syndrome, and pudendal nerve entrapment.3 Nevertheless, pudendal neuralgia remains relatively unknown. Medline search for “pudendal neuralgia” and “pudendal nerve entrapment” reveals only 51 peer-reviewed publications. “Pudendal neuropathy” yields more results, 115 publications, but few of them discuss diagnosis and treatment. Still, this syndrome if often unrecognized by the majority of physicians, including physicians experienced in pelvic pain such as gynecologists, urologists, and neurologists.
EPIDEMIOLOGY
The prevalence of pudendal neuralgia is unknown, although some have estimated a prevalence of 1/100,000 people. Spinosa et al.4 documented an incidence of 1% in the general population, affecting women more than men. Orphanet, www.ophra.net, a European website providing information about orphan drugs and rare diseases, states that pudendal neuralgia is diagnosed in 4% of patients undergoing treatment for chronic pelvic pain. However, from our experience, the incidence may be significantly higher, with women comprising 70% of our diagnosed patients.
SYMPTOMS
Pudendal neuralgia is described as a neuropathic pain in the distribution of the pudendal nerve.3 Pain may be present along the entire dermatome, or may be restricted to sites innervated by the nerve’s branches (Fig. 1). Pain may be localized to the clitoris, labia, vagina, and vulva in women, and to the penis and scrotum in men, excluding testes. In both sexes, pain may be localized to the perineum, rectum, and area immediately medial and anterior to ischial tuberosities. Symptoms are frequently unilateral, however, in patients presenting with bilateral pain, there is often a more affected side. Neuropathic pain is described as a burning, tingling, or itching sensation.5 Patients have significant hyperalgesia (increased sensitivity to mild painful stimuli), allodynia (pain in response to nonpainful stimuli), and parathesia (sensation of tingling or numbness). A small percentage of patients may have pain outside the area of innervation for the pudendal nerve, commonly presenting in the lower abdomen, posterior thigh, and lower back. This pain is usually attributed to muscle spasm or somatic referred pain.
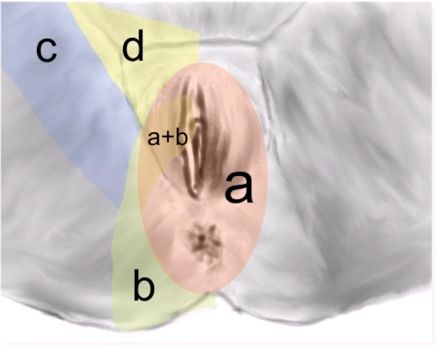
Fig. 1. Innervation of perineum. (a) Pudendal nerve, (b) inferior cluneal nerve, (c) obturator nerve, and (d) genitofemoral and ilioinguinal nerves
Typically, symptoms are present with sitting and absent during standing or lying down. However, with disease progression, the pain may become constant and severely aggravated by sitting. Most patients tolerate sitting for only several minutes before their pain becomes unbearable, and some are unable to sit at all. Interestingly, most patients report absence or improvement of pain when sitting on a toilet seat,6 as the body weight in this position is supported by the ischial tuberosities, thereby relieving pressure from the pelvic floor. Similarly, sitting on hard surfaces is more comfortable as well.
Another common symptom is the sensation of a foreign body in the vagina, perineum or rectum, frequently described as a “golf ball” or “tennis ball”. To help describe this sensation, we have coined the term “allotriesthesia” from the Greek allotri- (foreign) and esthesia (sensation). Defecation and urination can also be painful, leading to dyschezia and urinary hesitancy. Urinary or fecal incontinence may develop from decreased sphincter tone if motor function is affected.7 Patients with pudendal neuralgia are often diagnosed with interstitial cystitis,8 vulvodynia, dyspareunia, and persistent sexual arousal.9 Dyspareunia, pain with intercourse, can be so severe that patients are often unable to engage in sexual activity. Pain may be specific to arousal/erection, ejaculation, vaginal penetration, as well as orgasm. In contrast, pudendal neuralgia may also present as persistent sexual arousal, also called restless genital syndrome.9 It is a very unpleasant and sometimes painful sensation of intense arousal without the ability to climax. Unfortunately, this sensation remains constant, climax itself providing only momentary relief.
ANATOMY OF THE PUDENDAL NERVE
The pudendal nerve is derived from the sacral roots of S2–S4 and later divides into three branches, the dorsal clitoral/penile, the perineal, and the rectal.10 It carries motor, sensory and autonomic fibers. Injury to the pudendal nerve affects both afferent and efferent pathways, although sensory deficits are much more common than motor. The course of the pudendal nerve first emerges from the sacrum (S2–S4 sacral roots) and it travels laterally and inferiorly on the anterior surface of the piriformis muscle. After leaving the inferior edge of the piriformis muscle, it enters the gluteal region where it joins the pudendal artery and vein, which both accompany the nerve for the remainder of its course. This neurovascular bundle then travels inferiorly and posteriorly in the fixed space between the sacrospinous (anterior) and sacrotuberous (posterior) ligaments. At this point, the pudendal nerve is the most posterior (dorsal) structure, followed by the pudendal vein and pudendal artery that is most anterior. The neurovascular bundle then wraps around the posterior surface of the sacrospinous ligament and turns anteriorly and laterally. It then enters the aponeurosis of the obturator internus muscle, commonly called Alcock’s canal or the pudendal nerve canal (Fig. 2).

Fig. 2. Course of the pudendal nerve from the left posterior
The first major branch of the pudendal nerve is the inferior anal nerve or the rectal nerve. Its origin from the pudendal nerve is highly variable and may occur at the level of sacrospinous ligament, prior to entry into Alcock’s canal, in the canal itself, or after it exits the canal. The rectal branch of the nerve travels through the medial wall of the pudendal canal, along with the inferior rectal vessels. It crosses the ischioanal fossa to innervate the external anal sphincter, the distal anal canal, and the circum-anal skin. The cutaneous branches of the inferior rectal nerve distributed around the anus often overlap with the perineal branch of the posterior femoral cutaneous nerve and labial/scrotal nerves. The inferior rectal nerve occasionally arises directly from the sacral plexus and may reconnect with the pudendal nerve or run independently to the anus. In females the inferior rectal nerve may supply sensory branches to the lower vagina.
The second branch is the perineal nerve, which runs inferiorly in Alcock’s canal. It divides into posterior labial/scrotal (sensory) branches and muscular (motor) branches. The posterior labial/scrotal branches travel in the lateral part of the urogenital triangle and supply the skin of the labia majora or scrotum, overlapping with the distribution of the perineal branch of the posterior femoral cutaneous nerve and inferior rectal nerve. In females the posterior labial branches also supply sensory fibers to the skin of the lower vagina. Muscular branches of the perineal nerve supply the superficial transverse perineal muscle, bulbospongiosus, ischiocavernosus, deep transverse perineal muscle, sphincter urethrae and the anterior part of the external anal sphincter, and levator ani.
The third branch, dorsal clitoral/penile nerve, emerges from underneath the inferior ramus of the pubic bone and penetrates into the urogenital membrane. It then turns sharply cephalad, traveling between the ischiocavernosus muscle and inferior margin of the inferior pubic ramus. The nerve then makes a very sharp anterior turn entering the clitoris. It is here where the nerve begins dividing into its smaller terminal branches.
ANATOMICAL BASIS OF NERVE COMPRESSION
In general, nerves can be compressed in areas of fixation, acute flexion, and narrow canals. For that reason, the pudendal nerve can be compressed in several locations along its course. First, the nerve can be compressed as it emerges from underneath the piriformis muscle.11 Second, and most common, it may be compressed as it travels between the sacrospinous and sacrotuberous ligament. The third area of compression is Alcock’s canal. The fourth area of compression is where the dorsal nerve of the clitoris/penis emerges from underneath the inferior ramus of the pubic bone and turns cephalad. Finally, compression can occur when the dorsal nerve of the clitoris/penis makes an anterior turn to enter the clitoris/penis.
Injury of the nerve(s) may be uni- or bilateral, although unilateral injury seems to be more common. Indeed, it has also been hypothesized that pudendal nerve injury may be responsible for inducing an increase in the C-fiber pathway of the bladder, leading to urinary urge incontinence and to the development of overactive bladder syndrome.
POSTERIOR FEMORAL CUTANEOUS NERVE
Although the pudendal nerve is predominantly responsible for pelvic and perineal innervation, the posterior femoral cutaneous nerve (PFCN) also supplies sensory innervation to the perineum.12 The PFCN arises from the ventral rami of S1–S4 and courses with the pudendal nerve until it reaches the ischial tuberosity. At this level, the PFCN passes inferior to the ischial tuberosity to access the superficial fascia of the perineum. It then divides into the inferior cluneal and perineal nerve. The inferior cluneal nerve innervates the inferior buttock, while the perineal branch innervates the lateral perineum, proximal medial thigh, the posterior lateral aspect of the labium majus or scrotum, and the clitoris or penis. The perineal branch of the posterior femoral cutaneous nerve (PBPFCN) communicates with the inferior rectal nerve, and it is thought that this communication is the reason why sensory impairment is not seen with pudendal nerve entrapment.
Anatomically, the PFCN shares sensory innervation along the distribution of the pudendal nerve, and entrapment of the PFCN can lead to symptoms of pudendal neuralgia. Nevertheless, distinguishing symptoms include burning in the buttock, proximal medial thigh, and worsening pain when applying pressure to the ischial tuberosities such as sitting on a toilet seat. To differentiate pudendal neuralgia from PFCN entrapment, a CT guided block can be performed at the entrance to Alcock's canal to isolate the pudendal nerve. Failed alleviation of symptoms would suggest PFCN entrapment. Treatment for neuropathy of the PFCN consists of CT guided nerve blocks at the ischial spine to access the PFCN or an injection 4 cm inferior to the ischial tuberosity to block the PBPFCN. Surgical decompression can be an alternative treatment for failed conservative management.
MECHANISMS OF NEUROPATHIC PAIN
Neuropathic pain is commonly described as “pins and needles”, “burning”, “cold”, “numbness”, or “itching”. Symptoms are secondary to lesions directly affecting the somatosensory system. In healthy peripheral nerves, pain impulses are carried by unmyelinated nociceptive C-fibers and thin, myelinated A-delta fibers.5 Stimulation of C-fibers induces burning pain, while A-delta fibers are responsible for sharp, well-localized pain. When peripheral nerves are injured, abnormal regeneration can lead to spontaneous ectopic activity in sensory neurons. Thus, regenerating neurons become hypersensitive and develop pathological activity such as abnormal excitability and heightened sensitivity to chemical, thermal, and mechanical stimuli.5 This phenomenon is called peripheral sensitization.
CENTRAL SENSITIZATION
In contrast, central sensitization develops from increased responsiveness of neurons in the dorsal horn of the spinal cord.13 Increased intracellular calcium conducted by N-methyl-D-aspartate (NMDA) receptors enhances synaptic inputs by increasing the number of synapses on dorsal horn neurons. This enhancement leads to neuronal excitability, thereby responding to noxious and innocuous stimuli. Central sensitization also produces allodynia and hyperalgesia similar to peripheral sensitization.
Understanding this phenomenon is an important step in the successful treatment of pudendal neuralgia. Due to differences in pain pathways, peripheral sensitization is more responsive to surgical treatments compared with central sensitization. Central sensitization can be very difficult to reverse. Ketamine, an anesthetic used in pediatric and veterinary medicine, is used in the treatment of chronic pain and central sensitization.14 Detailed description of use of ketamine in treatment of chronic pelvic neuropathic pain is beyond the scope of this chapter, but several studies have shown its significant benefit in the treatment of chronic pain syndromes.15, 16
PUDENDAL NEURALGIA AND COMPLEX REGIONAL PAIN SYNDROME
Patients with severe pudendal neuralgia can develop complex regional pain syndrome (CRPS). CRPS is a condition, which may develop in 2–5% of all patients with peripheral nerve injuries.17 Previously known as reflex sympathetic dystrophy, it is a condition of sensory, autonomic, and motor dysfunction that occurs spontaneously (CRPS I) or after an identified nerve injury (CRPS II).
Complex regional pain syndrome
Smoking tobacco has been found to be strongly associated with development of CRPS. Symptoms include severe burning, edema, hyperhidrosis, increased hair growth, muscle spasms, swelling, changes in skin temperature and color, joint tenderness and restricted or painful joint movement. Patients also have allodynia, which is not limited to the territory of a single peripheral nerve.
It appears that CRPS II is caused by a physiological wind up and central nervous system sensitization, mediated by up-regulation of NMDA receptor. Intense or prolonged painful stimuli cause an exaggerated release of glutamate from peripheral nociceptive afferents located within dorsal horn neurons within the spinal cord. The glutamate then stimulates NMDA receptors on the second-order neurons, thereby producing the phenomena of central sensitization. Additional factors, such as cytokine release, exaggerated neurogenic sympathetic coupling and others, have been implicated in the pathophysiology of CRPS II. We believe that patients with pudendal neuralgia may progress in their symptomatology and develop CRPS II. Therefore, they may require treatments for both nerve compression and CRPS. This makes treatment of patients with CRPS and pudendal neuralgia significantly more complex than those with isolated nerve injury.
CAUSES OF PUDENDAL NEURALGIA
Pudendal neuralgia may arise from five distinct mechanisms. First, there may be a direct injury to the nerve. Second, pelvic floor muscles spasm, or pelvic floor tension myalgia, may cause compression of the nerve. Third, pelvic floor muscle spasm alone, without pudendal neuropathy, may also mimic pudendal neuralgia symptoms. Fourth, biochemical injury from infection or disease may occur. Finally, there may be compression of the spinal cord or nerve roots.
Mechanical injury occurs from compression, stretching or transection of the nerve. Compression, termed pudendal nerve entrapment, is the most common form of mechanical injury.18 Although the terms “pudendal nerve entrapment” and “pudendal neuralgia” have been used interchangeably, caution must be taken labeling patients with “pudendal nerve entrapment” without evidence of mechanical compression. Compression can be transient or permanent. Transient compression is caused by spasm of the surrounding muscles, most often the obturator internus muscle. In our practice we have also noticed there is a group of patients who develop pudendal pain after intense exercise programs, especially those including rapid flexion of the body at the trunk or from extensive use of the hip adductor fly machine. Permanent compression of the nerve is caused by adhesions or foreign bodies such as mesh or suture entrapping the nerve.19 Our clinical experience dictates it may be difficult to distinguish between patients who only have muscle spasms from those who have nerve injury. Indeed, patients with nerve injury almost always have accompanying muscle spasms; therefore it is paramount to separate both groups since treatment regimens are different (see diagnosis and treatment section).
Biochemical or nonmechanical causes of pudendal neuropathy are uncommon. Case reports, as well as evidence from our own clinical experience, confirm the development of pudendal neuralgia from viral infection (herpes zoster, HIV), diabetes, multiple sclerosis, and others.20 Treatment for this group of patients is directed toward treating the underlying disease. Nevertheless, neuralgia may persist even after treatment.
Historically, the first identified cause of pudendal neuralgia was cycling and it was initially called the “cyclist syndrome″ or “syndrome cycliste”.1, 21 This is a result of a mechanical compression of the nerve from prolonged pressure on Alcock’s canal and medial to ischial tuberosities leading to scarring. Nevertheless, in our practice, the most common injuries leading to pudendal neuralgia are pelvic surgery, traumatic falls on the buttock or back, or vaginal delivery with or without instrumentation. During vaginal delivery, pudendal nerve injury occurs from stretching of the pelvic floor by the fetal head at the level of the ischial spines.22 From our own preliminary data on 91 patients (75 women and 16 men) who underwent pudendal nerve decompression surgery, we found that 32 patients developed neuralgia after surgery, 14 after pelvic floor trauma, five after vaginal delivery, four after intense lower extremity exercise, and three after anal intercourse (Table 1). The remaining patients did not have an identifiable cause. Patients without a precipitating event often describe a gradual onset of pain, with intermittent episodes of pain in the perineum before typical symptoms of pudendal neuralgia emerged.
Table 1. Causes of pudendal neuralgia
1. Pelvic surgery especially with use of mesh |
2. Pelvic trauma |
3. Childbirth |
4. Bicycle riding |
5. Prolonged sitting |
6. Constipation |
7. Anal intercourse/use of anal devices |
8. Excessive masturbation |
The most common surgical procedure leading to pudendal neuralgia is repair of pelvic organ prolapse. Direct injury to the nerve can be seen after prolapse surgery including sacrospinous ligament fixation and mesh procedures. Pudendal neuralgia development after hysterectomy, anterior colporrhaphy or mid-urethral slings is more difficult to explain, although current theory purports that bleeding from the surgical procedure into Alcock’s canal can lead to scarring.23 Recent advances in magnetic resonance imaging (MRI) techniques have demonstrated the presence of vascular congestion in the pudendal neurovascular bundle after hysterectomy possibly applying pressure to the nerve directly. Nevertheless, it is very important to evaluate patients without evidence of direct injury to the pudendal nerve for other neuropathies and pelvic floor muscle spasm. Most patients report developing pudendal neuralgia symptoms immediately postoperatively. Unfortunately, this pain is frequently attributed to normal postoperative pain and the diagnosis goes unrecognized. Gradual onset of symptoms has also been reported in the weeks following surgery.
Clitoral or penile pain can develop from injury to the dorsal nerve of the clitoris/penis. Frequently, groin injury from bicycle seat, excessive masturbation, and infection, such as prostatitis or vestibulitis, are reported as inciting events. Entrapment of the dorsal nerve may occur from scar tissue, pelvic congestion, and spasm of the bulbocavernosus muscle. Treatment is directed toward the dorsal nerve with physical therapy, steroid injections, and/or transperineal decompression.
Tarlov cysts are meningeal cysts located in the sacral region. These cysts are usually considered incidental findings on MRI, but may cause sciatica or perineal pain resembling pudendal neuralgia. The incidence of Tarlov cysts in asymptomatic patients is approximately 4.6%, but is present in 17% of sciatica patients.24 Some studies suggest that up to 50% of patients with Tarlov cyst may have perineal pain.25 Symptomatic Tarlov cysts should correlate with their location. Symptoms worsen with increase in CSF pressure demonstrated by Valsalva maneuver. Pain is improved with lying down. Relief of symptoms after aspiration of the cyst is diagnostic.26 Surgical management usually includes extensive bony decompression with laminectomy, partial resection, and over-sewing of the cyst, or total cyst excision.
DIAGNOSIS OF PUDENDAL NEURALGIA
Pudendal neuralgia can be very difficult to diagnose, as no specific test exists.27 Therefore, diagnosis of this condition relies heavily on a proper history and physical examination.
History should first be directed at identifying symptoms of pudendal neuralgia (see section on symptoms). Then, an inciting event should be explored. It is very important to establish how and when the injury occurred, and whether symptomatology was immediate or gradual. Commonly, surgery, vaginal delivery, or pelvic trauma is identified. Pudendal nerve entrapment is rarely idiopathic. Therefore, if there is no identifiable event, causes other than pudendal nerve entrapment should be ruled out.
Physical examination should confirm pain is in the dermatome of the pudendal nerve.28 Sensation over this area may be assessed, although most patients will not have sensory defects. Skin perspiration or dryness is frequently identified on the affected side. A detailed examination of the back, abdomen, and pelvic floor muscles should be performed. The rectus abdominis, psoas major, levator ani, obturator internus, and coccygeus muscles are assessed for tenderness, strength, and spasm. Also, tenderness over the ischial spines and Alcock’s canal is consistent with pain originating from the pudendal nerve. Palpation of this area precipitates a tingling sensation commonly known as Tinel’s sign. Tinel’s sign may also be present when percussing the dorsal clitoral/penile branch as it emerges from underneath the inferior ramus of the pubic bone. Even after a detailed examination, it may be difficult to distinguish whether tenderness is caused by nerve injury or muscle spasm. In these cases, nerve blocks or Botox injections into the pelvic floor muscles may aid in the diagnosis of pudendal neuralgia.
One of the greatest authorities in surgical decompression of the pudendal nerve(s), Professor Roger Robert from Nantes, France, published his own criteria to diagnose pudendal neuralgia in 2008 (Table 2). These criteria have been validated27 and are based on the consensus of mostly European physicians with extensive experience treating pudendal neuralgia. The study showed that patients meeting all the required criteria have better outcomes from decompression surgery than patients who only partially meet them.
Table 2. Nantes criteria for the diagnosis of pudendal neuralgia
Inclusion criteria |
|
|
|
|
|
Exclusion criteria |
|
|
|
|
Complementary criteria |
|
|
|
|
|
|
|
|
Associated signs |
|
|
|
|
|
|
|
|
|
MRI, magnetic resonance imaging; CT, computed tomography; PNMTL, perineal branch of the posterior femoral cutaneous nerve
Tests used for diagnosing pudendal neuralgia include diagnostic blocks of the pudendal nerve(s), pudendal nerve motor terminal latency, sensory threshold testing, Doppler ultrasound, and functional MRI. Diagnostic pudendal nerve blocks are important Nantes inclusion criteria. These blocks can be performed unguided or with the use of image-guided techniques. Resolution of pain after the block, even if temporary, supports the diagnosis of pudendal neuralgia. These blocks also serve a very important therapeutic role, which will be described in the treatment section.
Unguided blocks in females are easily performed via a vaginal approach similar to the pudendal nerve block performed during labor. On the vaginal exam, the ischial spines are palpated and the injection is placed slightly medially and posteriorly to the ischial spines. The needle should penetrate the entire thickness of the sacrospinous ligament to access the nerve. In male patients, the pudendal nerve block can be performed transperineally. In this case, the ischial spine is palpated rectally and a needle is placed through the gluteal region lateral to the rectum and directed toward the ischial spine. The disadvantage of unguided pudendal nerve blocks is their inaccuracy and poor reproducibility. Failure of the procedure to alleviate pain may be due to operator error and not necessarily due to the absence of pudendal neuralgia. As a result, image guided blocks are preferred to support or rule out the diagnosis.
Image guided pudendal nerve blocks may be performed under fluoroscopy, ultrasound or CT scan. The first two are advantageous as they may be performed in the office setting, whereas CT scan requires a hospital or radiological facility. Injections under fluoroscopic guidance are performed with the patient in the prone position.26 A radiopaque needle is placed directly through the buttock and aimed toward the ischial spine. The injection is placed slightly medially and inferior to the ischial spine, similar to the transvaginal injection. Ultrasound guided injections can be performed transvaginally or transgluteally.29 The pudendal vessels are identified via Doppler imaging and the injection is placed immediately posterior to the vessels, in the area of the pudendal nerve. Blocks under CT guidance are performed transgluteally with the patient in the prone position.30 The advantage of CT guided injection is that it allows placement of the block into Alcock’s canal. Placing blocks into the Alcock’s canal allows differentiation between pudendal neuralgia and inferior cluneal neuralgia.
With properly performed blocks, patients may have relief of pain for hours to weeks. Longer efficacy can be achieved with steroid medications injected together with local anesthetics. The most commonly injected steroid is triamcinolone (Kenalog®) 40 mg per side. The addition of steroids decreases inflammation around the nerve, which may lead to improvement in pain.31 It has also been shown that steroids cause muscle atrophy leading to decreased pressure on the nerve. This steroid effect begins approximately 2 weeks from injection and may last from weeks to months.32
Pudendal nerve motor terminal latency (PNMTL) measures conduction velocity of electrical impulses through the pudendal nerve.31, 33 Electrical impulses are applied transvaginally or transrectally at the level of the ischial spine and the time needed for the impulse to travel to the perineal muscles is measured. The simplest way to measure latency is by using a St Mark’s electrode. This electrode is taped on a glove with a stimulating cathode at the tip of the index finger and return anode at the base of the same finger. The digit covered with this electrode is inserted vaginally or rectally and an impulse is applied to the nerve at the ischial spine. Time necessary for the impulse to travel through the nerve to pelvic floor muscles is measured. Values that are considered to be normal are less than 3.5 milliseconds in nulliparous patients. Unfortunately PNMTL values in patients with previous vaginal delivery or pelvic surgery are highly variable due to pelvic floor muscle stretching.34, 35 Also, PNMTL measurements have very high intra- and interobserver variability.36 Thus, the PNMTL is considered by most experts to be too inconsistent for the diagnosis of pudendal neuralgia. More accurate tests, in which the return electrode needle is placed directly into the transverse perineal muscle, have been developed. However, their accuracy regarding diagnosis of pudendal nerve entrapment is still under investigation.
Quantitative sensory threshold testing is an important concept in diagnosing peripheral nerve injury.37 The premise of this test is that compressed nerves lose the ability to transmit sensation of temperature changes and vibration. The most commonly used test is the warm detection threshold test. A probe is applied to the area of innervation of the surveyed nerve and temperature is then slowly raised. Patients with nerve injury cannot detect gradual temperature changes and can only react to high temperature when it becomes a painful stimulus.
Another way to diagnose neuropathic pain is pressure sensory testing. This test relies on the patient’s ability to distinguish pressure thresholds between affected and unaffected sides. A probe is applied to patients’ skin and pressure is gradually increased; patients indicate when pressure is felt. In two-point discrimination testing, the distance between the two probes (pressure points) is increased and patients are instructed to indicate when two points are distinctly felt. It has been shown that pressure sensory testing results differ significantly between the affected and unaffected side, and that results improve after successful treatments.38 Similarly, compressed nerves lose their ability to transmit stimuli of vibration that can be detected by tuning forks or similar devices.
High frequency ultrasound (15 MHz linear probe) is often used to diagnose compression and pathology of peripheral nerves. Inflamed nerves that are not compressed may appear edematous with increased blood flow and enlarged.39 In contrast, compressed nerves will appear flat. Unfortunately, pudendal nerves are positioned deep in the pelvis and only the terminal branches such as the dorsal nerve of the clitoris (penis) can be seen by ultrasound.
Doppler ultrasound has been advocated as a test to diagnose pudendal nerve entrapment.39, 40 Because the nerve courses together with the pudendal artery and vein in a neurovascular bundle, it is hypothesized that compression of the nerve would lead to compression of the vein. During surgery, varicosities of this vein are often encountered in the area of nerve compression. Doppler ultrasound has the ability to detect a gradient in venous flow around the area of compression.
Functional MRI detects tissues based on their biological properties and not on their anatomical differences.41 The method applied in assessment of nerve integrity is called “diffusion tensor imaging”. It relies on the ability of water to diffuse more rapidly along nerve fibers rather than perpendicularly. Together, with three-dimensional imaging and advanced computer algorithms, this method may be the future of the diagnosis of pudendal neuralgia. In its current state, this imaging modality does not seem to be accurate enough to diagnose pudendal nerve compression and is viewed as experimental and inconclusive by most.
Until recently, there were no specific radiological findings in patients with pudendal nerve entrapment.27 Advances in MRI, allow for good visualization of the main trunk of the nerve and terminal branches. Currently there are two centers in the United States that perform these highly specialized scans (New York, NY and Phoenix, AZ). In our practice, this imaging modality has tremendously changed the way we diagnose pudendal nerve entrapment. It has been our experience that MRI findings have a good correlation with findings during transgluteal decompression surgery. Nevertheless, more research is necessary to determine its validity.
TREATMENT OF PUDENDAL NEURALGIA
Conservative therapy
The mainstay treatment of pudendal neuralgia is conservative therapy.42 Avoidance of injury and pain related to pudendal neuralgia is an important element of treatment. Patients who developed pain as a result of specific exercises such as cycling or adduction should cease immediately. If pain is present with prolonged sitting, lifestyle changes and work environment modifications should be implemented to minimize sitting. If sitting cannot be eliminated, patients should use a cushion that supports the ischial tuberosities to elevate the pelvic floor off the seat. This support decreases the pressure applied to the pelvic floor muscles and pudendal nerve. Pain can cause spasm of the pelvic floor muscles and lead to increases in pressure on the nerve and a subsequent increase in pain levels. This vicious cycle is often very difficult to break and may lead to peripheral and central sensitization of pain. From our experience, we believe that approximately 20–30% of patients get better with lifestyle modifications.
Medical therapy can be used in patients who fail lifestyle modifications. The three most important groups of medications used in treatment are muscle relaxants, anticonvulsants, and analgesics.6 There are no available studies investigating medical management. In our practice, the muscle relaxants we find most useful are a twice-daily valium 5 mg and baclofen 4 mg vaginal or rectal suppository. Oral muscle relaxants are not as effective, however, Zanaflex® 2 mg twice a day seems to work better than others. Gabapentin (Neurontin®) and pegabalin (Lyrica®) are used to treat neuropathic pain. Both medications are gamma aminobutyric acid (GABA) analogues, which were synthesized to mimic this neurotransmitter. Gabapentin binds to the α2δ subunit of voltage-dependent calcium channels in the central nervous system. It has been proven that gabapentin halts the formation of new synapses therefore decreasing neuropathic pain.43 Pregabalin is a drug that is related in structure to gabapentin. Compared with gabapentin, pregabalin is more potent, absorbs faster and has greater bioavailability.44 Higher potency leads to fewer dose related adverse effects. Use of both gabapentin and pregabalin for treatment of pudendal neuralgia is not FDA approved, although it is clearly beneficial in reducing pain. The usual starting dose for Neurontin is 300–900 mg/day in three divided doses, titrated up to maximum 3600 mg/day. Lyrica is usually started at 75 mg twice a day. Doses may be increased to a maximum of 600 mg/day in two to three divided doses.
In patients with muscle spasms, pelvic floor physical therapy is the gold standard treatment. It can help distinguish myalgia from neuralgia. The main role of physical therapy is relaxation of the pelvic floor muscles. Therapists address spams, muscle imbalances, restricted connective tissues, and other dysfunctions. Therapy is administered as “hands-on” techniques, focusing on posture, range of motion, exercises, stretching, and education. Most of these patients have significant muscle spasm and subsequent muscle shortening throughout the pelvic girdle. Manual techniques that help release muscle spasm and lengthen the muscle include myofascial release, soft and connective tissue mobilization, and trigger point release. Other modalities include biofeedback, ultrasonography, and electrical stimulation.
In patients who show no improvement in pelvic floor muscle spasm, botulinum toxin injection into the pelvic floor is a good treatment alternative. Administered doses between 50 and 400 units of Botox® are reported in the literature.45 In our practice we use 200 units of botulinum toxin diluted in 20 ml of normal saline. Approximately 20 injections are done uni- or bilaterally using a pudendal nerve block needle. This procedure is done in the operating room under anesthesia. Care has to be taken not to inject Botox into the anal or urinary sphincter as it may cause transient incontinence. After 5–7 days, patients should resume physical therapy. In our practice, we found that 67% of patients with pelvic floor tension myalgia benefit from botulinum toxin an injection, but the success rate falls to 30% when performed specifically for pudendal neuralgia.
Steroid injections to pudendal nerve(s)
Local anesthetic and steroid injections around the pudendal nerves are important treatment modalities in patients with neuralgia. Injections may be performed unguided and transvaginal in women, or image guided by fluoroscopy, ultrasound, or CT scan in both sexes. CT scan guided nerve blocks are thought to be the most accurate and reproducible method. In a recent study by Fannuci et al.,46 27 patients with pudendal neuralgia underwent CT guided pudendal nerve blocks. At 1-year follow-up, 92% showed continued clinical improvement. In our clinical experience, long-term benefits are seen 25–30% of patients.
Surgical treatment of pudendal neuralgia
Surgical decompression is the treatment of choice in patients with pudendal nerve entrapment. Proper patient selection is paramount, as treatment success is highly dependent on an accurate diagnosis. There are four described approaches to surgical decompression of the pudendal nerve. All surgical methods involve neurolysis to eliminate the possible source of compression.
TRANSPERIANAL
The transperianal approach was originally described by Shafik et al. in Egypt.47 This approach was originally developed to treat fecal incontinence. Patients are positioned in dorsal lithotomy position. A semicircular incision is made on the side of the anus on which the nerve is affected. The surgeon then identifies the inferior rectal nerve and follows it blindly with a finger until the pudendal nerve is reached. Adhesions around the pudendal nerve are then bluntly reduced. This approach allows access to the rectal branch and should be limited to patients with only rectal involvement of pudendal neuralgia. Although one of the least invasive approaches, it is a blind procedure that does not allow for extensive dissection of the nerve beyond the distal Alcock’s canal.
TRANSGLUTEAL
The transgluteal decompression is currently the most common and successful approach for pudendal neurolysis. This procedure was originally described by Professor Roger Robert from Centre Hospitalier Universitare in Nantes, France.11, 48, 49 The patient is positioned in prone jackknife position. A transgluteal incision is made in the location overlying the sacrotuberous ligament. When the ligament is reached, it is transected at its narrowest portion and edges of the ligament are reflected open. The pudendal nerve is found immediately below the ligament together with the pudendal vein and artery. Through this approach, the nerve can be visualized from the subpiriformis fossa to the distal Alcock’s canal. Neurolysis is performed and the sacrospinous ligament is transected. The nerve is then transposed anteriorly to decrease tension. Surgery is concluded by the closure of the subcutaneous fat and overlying skin. In a sequential randomized control trial, 71.4% of the surgery group compared with 13.3% of the nonsurgery group had improved at 12 months.50
In our practice, we have made several modifications to the procedure. A high power surgical microscope and Nerve Integrity Monitoring System (NIMS, Medtronics) is used to identify the pudendal nerve. After neurolysis Neuragen (Integra), a nerve-protecting wrap, is placed around the nerve to prevent formation/reformation of scar tissue. The nerve is also coated with activated platelet plasma, which contains growth factors promoting nerve healing.51 Before closure, a pain pump catheter is placed along side the nerve infusing 0.5% bupivacaine at 2 ml/h for 10–14 days postoperatively. Continuous infusion of bupivacaine provides excellent anesthesia after surgery and allows patients to be more mobile. We also believe that preventing pain impulses from operated nerves decreases the risk of developing central sensitization and complex regional pain syndrome. Finally, there is evidence that bupivacaine prevents proliferation of fibroblasts therefore directly reducing the risk of scar formation.52
Another modification is the repair of the sacrotuberous ligament. There is an ongoing argument whether the sacrotuberous ligament provides any significant stability to the sacroiliac joint and hopefully future research will answer this question. Opponents of ligament repair believe that a reconstructed ligament may increase the risk of adhesions leading to future entrapment of the nerve. We believe that repaired ligament provides stability to the sacroiliac ligament, and risk of adhesions is minimized by the use of Neuragen. In our patient population, we have found that 70% of patients have improvement in pudendal neuropathic pain. Patients may still have pain related to muscle spasms, which requires ongoing treatment with physical therapy or botulinum toxin.
TRANSISCHIORECTAL
The transischiorectal approach was developed by Eric Bautrant from Aix-en-Provence, France, in order to avoid the need FOR transection of the sacrotuberous ligament.53 In this technique, an incision is made in the lateral wall of the vagina in women and between the rectum and the scrotum in men. Dissection is then directed to the ischiorectal fossa on the affected side. Electromyogram is used to direct the surgeon to the area of compression to limit the need of extensive dissection. Similarly to the transperinal approach, access to the pudendal nerve is limited. Recovery is difficult in men with painful incisions between the scrotum and rectum that are prone to infection. Bautrant initially reported 86% improvement in pain 12 months after surgery.53 Unfortunately, experience in the United States has not been able to reproduce successful outcomes and thus this approach has fallen out of favor.
LAPAROSCOPIC
The laparoscopic approach has been advocated by Alfredo Nieves from Chattanooga, Tennessee (personal communication). This approach does not require transection of the sacrotuberous ligament and provides good visualization of the nerve’s course. Unfortunately, outcomes of laparoscopic decompression have been poor, thus, the procedure has been abandoned. It is possible that with introduction of robotic surgery, which allows greater visualization and precision, endoscopic procedures may again become an option for pudendal nerve decompression.
SUMMARY
Pudendal neuralgia is a painful neuropathic condition involving the dermatome of the pudendal nerve. It should be suspected in patients complaining of burning pain in the clitoris/penis, vulva/scrotum, perineum, and rectum. Pain is more severe with sitting, and relieved or improved by standing. Onset is usually immediately after vaginal surgery, pelvic trauma, or childbirth. The Nantes criteria are used for the diagnosis of pudendal neuralgia. CT guided pudendal nerve blocks are more precise than transvaginal injections for diagnosis. Initial therapies include minimizing activities that worsen the pain and pain medications. Physical therapy and Botox injections are used in patients identified with pelvic floor tension myalgia. When conservative treatments fail, transgluteal decompression should be performed (Fig. 3). Knowledge and best practice in this field are changing rapidly; therefore changes in diagnosis and treatment protocols are expected.
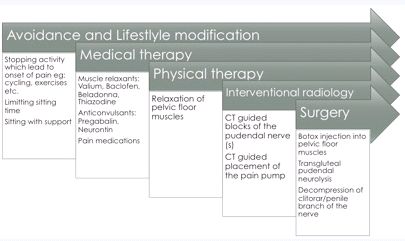
Fig. 3. Progression of treatments for pudendal neuralgia
St Joseph's Hospital and Medical Center
Based on available data and our clinical experience, we consider pudendal neuralgia to be multifactorial, involving not only compression of the pudendal nerve, but also muscle spasm, and peripheral and central sensitization. Initial evaluation of all our patients involves a detailed history and physical examination. Patients then receive a comprehensive evaluation by our physical therapist who has extensive experience with pudendal neuralgia. She evaluates the patients’ pelvic floor muscles and makes recommendations based on the extent of muscular involvement. Next, an MRI of the pelvis is obtained to evaluate for radiological evidence of compression.
Patients are then given tips for avoidance and counseled on lifestyle modification. Valium 5 mg/baclofen 4 mg vaginal or rectal suppositories and Lyrica 75 mg twice daily are prescribed. Patients who have primarily pelvic floor tension myalgia undergo physical therapy. If no improvement is seen after 6 weeks of therapy and muscles continue to be in spasm, Botox injection into the pelvic floor muscles is performed. This procedure is used to help differentiate neuropathic pain from muscle spasm.
CT guided blocks of the pudendal nerve are used for diagnosis and treatment in patients without significant pelvic floor muscle spasm or for patients who have failed physical therapy and Botox treatments. We routinely perform three injections of bupivacaine and 40 mg of triamcinolone 6 weeks apart before determining treatment failure. Patients with evidence of pudendal nerve compression on MRI are still offered nonsurgical therapy. If conservative therapy fails, patients are scheduled for transgluteal decompression of the pudendal nerve.
In patients with pain localized to the clitoris or penis, local injection of the dorsal nerve is performed under ultrasound guidance. Also, patients are offered a modified transperineal approach to decompression of the dorsal nerve. For patients with central sensitization, symptoms may continue after all interventions. Therefore, we are currently establishing a protocol for ketamine infusions.
It is our experience that patients require life-long lifestyle modification and therapy. Thus, our goal is to tailor a treatment plan to improve overall quality of life.
DISCLAIMER
Pudendal neuralgia and pudendal nerve entrapment are largely unknown conditions. There is a paucity of research on this topic. Information presented in this chapter is based on available peer-reviewed literature and our clinical experience from treating over 500 patients with pudendal neuralgia.
REFERENCES
Amarenco G, Lanoe Y, Perrigot M, Goudal H. [A new canal syndrome: compression of the pudendal nerve in Alcock's canal or perinal paralysis of cyclists]. Presse Med 1987;16(8):399. |
|
Amarenco G, Lanoe Y, Ghnassia RT, Goudal H, Perrigot M. [Alcock's canal syndrome and perineal neuralgia]. Rev Neurol (Paris) 1988;144(8-9):523-6. |
|
Amarenco G, Savatovsky I, Budet C, Perrigot M. [Perineal neuralgia and Alcock's canal syndrome]. Ann Urol (Paris) 1989;23(6):488-92 |
|
Spinosa JP, de Bisschop E, Laurencon J, Kuhn G, Dubuisson JB, Riederer BM. [Sacral staged reflexes to localize the pudendal compression: an anatomical validation of the concept]. Rev Med Suisse 2006;2(84):2416-8, 20-1 |
|
Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron 2006;52(1):77-92. |
|
Hibner M, Desai N, Robertson LJ, Nour M. Pudendal neuralgia. J Minim Invasive Gynecol 2010;17(2):148-53 |
|
Shafik A, El Sibai O, Shafik IA, Shafik AA. Role of sacral ligament clamp in the pudendal neuropathy (pudendal canal syndrome): results of clamp release. Int Surg 2007;92(1):54-9. |
|
Hansen HC. Interstitial cystitis and the potential role of gabapentin. South Med J 2000;93(2):238-42. |
|
Waldinger MD, Venema PL, van Gils AP, Schweitzer DH. New insights into restless genital syndrome: static mechanical hyperesthesia and neuropathy of the nervus dorsalis clitoridis. J Sex Med 2009;6(10):2778-87. |
|
Gray H, Williams PL, Bannister LH. Gray's anatomy : the anatomical basis of medicine and surgery. 38th ed. New York: Churchill Livingstone; 1995. |
|
Robert R, Prat-Pradal D, Labat JJ, et al. Anatomic basis of chronic perineal pain: role of the pudendal nerve. Surg Radiol Anat 1998;20(2):93-8. |
|
Darnis B, Robert R, Labat JJ, et al. Perineal pain and inferior cluneal nerves: anatomy and surgery. Surg Radiol Anat 2008;30(3):177-83. |
|
Bradley WG. Neurology in clinical practice. 5th ed. Philadelphia, PA: Butterworth-Heinemann/Elsevier; 2008. |
|
Goldberg ME, Domsky R, Scaringe D, et al. Multi-day low dose ketamine infusion for the treatment of complex regional pain syndrome. Pain Physician 2005;8(2):175-9. |
|
Hewitt DJ. The use of NMDA-receptor antagonists in the treatment of chronic pain. Clin J Pain 2000;16(2 Suppl):S73-9. |
|
Pozzi A, Muir WW, Traverso F. Prevention of central sensitization and pain by N-methyl-D-aspartate receptor antagonists. J Am Vet Med Assoc 2006;228(1):53-60. |
|
Hsu ES. Practical management of complex regional pain syndrome. Am J Ther 2009;16(2):147-54 |
|
Ramsden CE, McDaniel MC, Harmon RL, Renney KM, Faure A. Pudendal nerve entrapment as source of intractable perineal pain. Am J Phys Med Rehabil 2003;82(6):479-84. |
|
Fisher HW, Lotze PM. Nerve injury locations during retropubic sling procedures. Int Urogynecol J Pelvic Floor Dysfunct;22(4):439-41. |
|
Howard EJ. Postherpetic pudendal neuralgia. Jama 1985;253(15):2196. |
|
Leibovitch I, Mor Y. The vicious cycling: bicycling related urogenital disorders. Eur Urol 2005;47(3):277-86; discussion 86-7. |
|
Lien KC, Morgan DM, Delancey JO, Ashton-Miller JA. Pudendal nerve stretch during vaginal birth: a 3D computer simulation. Am J Obstet Gynecol 2005;192(5):1669-76. |
|
Corona R, De Cicco C, Schonman R, Verguts J, Ussia A, Koninckx PR. Tension-free Vaginal Tapes and Pelvic Nerve Neuropathy. J Minim Invasive Gynecol 2008;15(3):262-7. |
|
Acosta FL, Jr., Quinones-Hinojosa A, Schmidt MH, Weinstein PR. Diagnosis and management of sacral Tarlov cysts. Case report and review of the literature. Neurosurg Focus 2003;15(2):E15. |
|
Wilkinson HA. Tarlov cysts. J Neurosurg 2002;97(2 Suppl):271; author reply -2 |
|
Choi SS, Lee PB, Kim YC, Kim HJ, Lee SC. C-arm-guided pudendal nerve block: a new technique. Int J Clin Pract 2006;60(5):553-6 |
|
Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol Urodyn 2008;27(4):306-10. |
|
Labat JJ, Robert R, Delavierre D, Sibert L, Rigaud J. [Symptomatic approach to chronic neuropathic somatic pelvic and perineal pain]. Prog Urol;20(12):973-81. |
|
Peng PW, Tumber PS. Ultrasound-guided interventional procedures for patients with chronic pelvic pain - a description of techniques and review of literature. Pain Physician 2008;11(2):215-24. |
|
Thoumas D, Leroi AM, Mauillon J, et al. Pudendal neuralgia: CT-guided pudendal nerve block technique. Abdom Imaging 1999;24(3):309-12. |
|
Labat JJ, Robert R, Bensignor M, Buzelin JM. [Neuralgia of the pudendal nerve. Anatomo-clinical considerations and therapeutical approach]. J Urol (Paris) 1990;96(5):239-44. |
|
Filippiadis DK, Velonakis G, Mazioti A, et al. CT-guided percutaneous infiltration for the treatment of Alcock's neuralgia. Pain Physician;14(2):211-5. |
|
Le Tallec de Certaines H, Veillard D, Dugast J, et al. [Comparison between the terminal motor pudendal nerve terminal motor latency, the localization of the perineal neuralgia and the result of infiltrations. Analysis of 53 patients]. Ann Readapt Med Phys 2007;50(2):65-9 |
|
Olsen AL, Ross M, Stansfield RB, Kreiter C. Pelvic floor nerve conduction studies: establishing clinically relevant normative data. Am J Obstet Gynecol 2003;189(4):1114-9. |
|
Snooks SJ, Swash M, Henry MM, Setchell M. Risk factors in childbirth causing damage to the pelvic floor innervation. Int J Colorectal Dis 1986;1(1):20-4. |
|
Tetzschner T, Sorensen M, Rasmussen OO, Lose G, Christiansen J. Reliability of pudendal nerve terminal motor latency. Int J Colorectal Dis 1997;12(5):280-4. |
|
Walk D, Sehgal N, Moeller-Bertram T, et al. Quantitative sensory testing and mapping: a review of nonautomated quantitative methods for examination of the patient with neuropathic pain. Clin J Pain 2009;25(7):632-40 |
|
Greenspan JD. Quantitative assessment of neuropathic pain. Curr Pain Headache Rep 2001;5(2):107-13. |
|
Beco J, Mouchel J, Mouchel T, Spinosa JP. Concerns about the use of colour doppler in the diagnosis of pudendal nerve entrapment. Pain 2009;145(1-2):261; author reply 2. |
|
Mollo M, Bautrant E, Rossi-Seignert AK, Collet S, Boyer R, Thiers-Bautrant D. Evaluation of diagnostic accuracy of Colour Duplex Scanning, compared to electroneuromyography, diagnostic score and surgical outcomes, in Pudendal Neuralgia by entrapment: a prospective study on 96 patients. Pain 2009;142(1-2):159-63. |
|
Filler AG, Haynes J, Jordan SE, et al. Sciatica of nondisc origin and piriformis syndrome: diagnosis by magnetic resonance neurography and interventional magnetic resonance imaging with outcome study of resulting treatment. J Neurosurg Spine 2005;2(2):99-115. |
|
Benson JT, Griffis K. Pudendal neuralgia, a severe pain syndrome. Am J Obstet Gynecol 2005;192(5):1663-8 |
|
Magnus L. Nonepileptic uses of gabapentin. Epilepsia 1999;40 Suppl 6:S66-72; discussion S3-4. |
|
Johannessen Landmark C. Antiepileptic drugs in non-epilepsy disorders: relations between mechanisms of action and clinical efficacy. CNS Drugs 2008;22(1):27-47 |
|
Abbott J. Gynecological indications for the use of botulinum toxin in women with chronic pelvic pain. Toxicon 2009;54(5):647-53. |
|
Fanucci E, Manenti G, Ursone A, et al. Role of interventional radiology in pudendal neuralgia: a description of techniques and review of the literature. Radiol Med 2009;114(3):425-36. |
|
Shafik A, el-Sherif M, Youssef A, Olfat ES. Surgical anatomy of the pudendal nerve and its clinical implications. Clin Anat 1995;8(2):110-5. |
|
Robert R, Labat JJ, Riant T, Khalfallah M, Hamel O. Neurosurgical treatment of perineal neuralgias. Adv Tech Stand Neurosurg 2007;32:41-59. |
|
Robert R, Labat JJ, Riant T, Louppe JM, Hamel O. [The pudendal nerve: clinical and therapeutic morphogenesis, anatomy, and physiopathology]. Neurochirurgie 2009;55(4-5):463-9. |
|
Robert R, Labat JJ, Bensignor M, Pascal G, Deschamp C, Raoul S, Olivier H. Decompression and transposition of the pudendal nerve in pudendal neuralgia: a randomized controlled trial and long-term evaluation. European Urology 2004;47(3):403-8. |
|
Sariguney Y, Yavuzer R, Elmas C, Yenicesu I, Bolay H, Atabay K. Effect of platelet-rich plasma on peripheral nerve regeneration. J Reconstr Microsurg 2008;24(3):159-67. |
|
Maurice JM, Gan Y, Ma FX, Chang YC, Hibner M, Huang Y. Bupivacaine causes cytotoxicity in mouse C2C12 myoblast cells: involvement of ERK and Akt signaling pathways. Acta Pharmacol Sin;31(4):493-500. |
|
Bautrant E, de Bisschop E, Vaini-Elies V, et al. [Modern algorithm for treating pudendal neuralgia: 212 cases and 104 decompressions]. J Gynecol Obstet Biol Reprod (Paris) 2003;32(8 Pt 1):705-12. |